Collaborative Client Care
Initial Care of Client with a Burn and Collaboration
Breathing
Circulation
- Assess client - A,B,C’s
- Assess Body Surface area burned
- Assess location of burn
- Assess depth of burn
- Assess burn severity
- Assess other body systems
- Fluid resuscitation
- Medication and Pain management
- Members of the Burn Team
- If you can safely do so, remove client from source of burn (if they are not already removed)
- If this is a chemical burn, brush off chemical (wear PPE) or wash off with water if safe. If unsure, call poison control.
- Assess client based on ABC’s
Breathing
Circulation
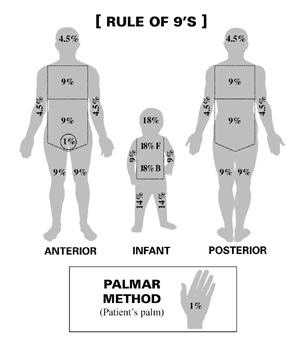
To Estimate Body Surface Area Burned Use the Following Methods:
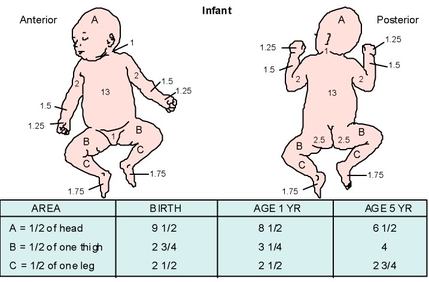
Accounts for a larger head
- Rule of 9’s
- Palmar Method
- Lund and Browder
Accounts for a larger head
|
|
Assess Location of Burn
Assess Depth of Burn (See Charts Below)
- If burn is located on head, neck or chest, frequently assess respiratory status
- Circumferential burns: circulatory status
- Look for signs and symptoms of an inhalation injury
Assess Depth of Burn (See Charts Below)
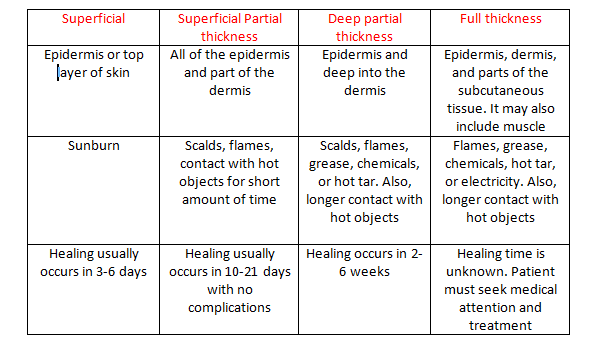

Image retrieved from: http://my.firefighternation.com/forum/topics/889755:Topic:2902596
Assess Severity of Burn
Under 10 years of age or over 50
Clients who have other injuries associated with the burn
Those who are immunocompromised
Electric or inhalation injury
History of cardiac, pulmonary, or chronic metabolic disorders
Burn is located on dominant hand, eyes, ears, face, feet, or groin area
Burns account for more than 25% total body surface area
Full thickness burn greater than 10% of total body surface area
Other Body Systems Involved
Increased heart rate
Damage from inhalation injuries may occur - Upper airway injuries may cause closing of the vocal cords
Alveoli damage/edema may occur from leaking capillaries
Burns may prevent chest from functioning which decreases lung expansion
Respirations increase
Bowel activity decreases
Distention of abdomen
Nausea/vomiting
Fluid Resuscitation
D5W
0.9% Normal Saline
Medication and Pain Management
This includes insulin. Administer IV medications as needed.
Members of the Burn Team
- Determine if the client is in the high risk population
Under 10 years of age or over 50
Clients who have other injuries associated with the burn
Those who are immunocompromised
- Criteria for burn center
Electric or inhalation injury
History of cardiac, pulmonary, or chronic metabolic disorders
Burn is located on dominant hand, eyes, ears, face, feet, or groin area
Burns account for more than 25% total body surface area
Full thickness burn greater than 10% of total body surface area
Other Body Systems Involved
- Fluid and electrolytes: fluid shifts occur which cause fluid to leak into the interstitial space. This is also known as capillary leak syndrome or third spacing. This decreases blood volume and pressure.
- During the first stage of burn care, hypovolemia, metabolic acidosis, hyperkalemia and hyponatremia can occur because of the fluid shift.
- The adrenal glands begin to secrete extra catecholamines and aldosterone.
- Metabolic rate and caloric needs increase because of wound healing.
- Blood sugar level rises.
- Decreased urinary output
- Cardiac:
Increased heart rate
- Pulmonary:
Damage from inhalation injuries may occur - Upper airway injuries may cause closing of the vocal cords
Alveoli damage/edema may occur from leaking capillaries
Burns may prevent chest from functioning which decreases lung expansion
Respirations increase
- Gastric:
Bowel activity decreases
Distention of abdomen
Nausea/vomiting
Fluid Resuscitation
- Use isotonic fluid at room temperature
D5W
0.9% Normal Saline
- Parkland formula to determine amount of fluid used to replace: 4mL*wt(kg)*%Body surface area burned
- Infuse ½ of the volume of fluid in the first 8 hours (Calculate this from time of the burn) and infuse the second ½ over the next 16 hours
- Cardiac output should return to normal within 18-36 hours
- Monitor urine output during fluid resuscitation: Adult: 30-50cc per hour
Medication and Pain Management
- Do not administer IM or SubQ medication
This includes insulin. Administer IV medications as needed.
- Burn victims will be in a lot of pain. It is important to provide pain relief with analgesics or morphine sulfate
- Evaluate tetanus status. If patient has not received a tetanus vaccine within the last 10 years administer one
Members of the Burn Team
- Nurses and nursing assistants: Both are involved in personal care of the client. Nurses are responsible for administering medication and wound care. Nursing assistants will help the client with ADL’s and personal care.
- Respiratory therapists: These are responsible for ventilator management. They work closely with the nurse to manage the client’s airway and restore respiratory function in the client.
- Wound care: These are responsible for working with the nurse to treat the wounds causes by burn injuries. They will assess and sometimes redress the wound. They also make treatment recommendations to aid in the healing of the wound.
- Case managers and social workers: Are involved in the psychosocial assessment of burn clients. They will help the client to address discharge options, home assistance, transportation and the ability to cope with the change in life.
- Chaplain: The client may ask for spiritual assistance during his/her hospital stay.
- Dietician: Nutrition is important in the wound healing purpose. A dietician will help to create a diet that is specific to the client.
- Occupational therapist: Are responsible for helping the client with range of motion exercises, positioning, and helping the client restore as much function as possible. They will assist the client to find ways to perform ADL’s and other desired activities.
- Physical therapist: Are responsible for therapeutic exercises, increasing muscle tone and pre-injury function. They will help the client by creating exercise programs and activities to help the client build strength and the ability to function as close to pre-injury level of functioning as possible
- Physicians: Are responsible for working with the team listed above to help the client return to their pre-injury life style, if possible. If not, they help the client to restore as much function as possible. Physicians can decide pain management and the type of wound dressings used. They may also perform procedures to aid in the wound healing process.
